

COMPARISON OF NASALANCE SCORES IN UPRIGHT, SEMI-UPRIGHT AND SUPINE POSITIONS IN HEALTHY INDIVIDUALS
2Tarsus University, Faculty of Health Sciences, Department of Speech and Language Therapy, Mersin, Türkiye
Summary
Objective: This study aimed to compare nasalance scores in three different body positions-upright, semi-upright, and supine-in healthy individuals. Understanding the impact of gravity and body positioning on velopharyngeal function during speech can provide insights into optimal assessment conditions, particularly in contexts like resonance disorders and velopharyngeal dysfunction surgeries.Material and Methods: A total of 70 native Turkish-speaking participants aged 20-52 were included. Nasalance scores were measured using a Nasometer II in three positions: supine, semi-upright, and upright. The assessment involved three speech passages representing oral, oronasal, and nasal phonetic contexts. Data were examined through Friedman tests and Wilcoxon signed-rank tests with Bonferroni corrections to identify significant differences between positions.
Result: Significant differences in nasalance scores were observed in nasalance scores between the supine and semi-upright positions across all phonetic contexts (p<.001). The upright position also exhibited notable differences compared to the supine position in oral and oronasal passages, suggesting that posture affects nasalance scores.
Conclusion: Body positioning significantly influences nasalance scores in healthy individuals. The results suggest that speech assessments and decisions regarding velopharyngeal dysfunction surgeries should consider the body position to ensure functional and reliable results, particularly in clinical settings where upright posture might better represent natural speech production conditions.
Introduction
The effects of gravity on living organisms have been the subject of numerous studies[1]. Gravity has a facilitating effect on various motor skills, such as walking and sitting. However, the impact of gravity on speech is a field that has been relatively under-researched. Several researchers have investigated the effect of gravity on velopharyngeal structures in both children and adults[2-5]. These studies have explored the impact of body position on velopharyngeal structures, with varied results due to differing methodologies and small sample sizes.The velopharyngeal mechanism plays a critical role in many functions, including speech. Velopharyngeal closure occurs during the production of oral speech sounds and some non-speech activities through the movement of the velum and pharyngeal walls[6]. Velopharyngeal dysfunction arises when the velopharyngeal mechanism fails to function properly for various reasons. During surgeries for velopharyngeal dysfunction, physicians may evaluate the velopharyngeal region using videofluoroscopy, nasopharyngoscopy, or magnetic resonance imaging (MRI). MRI imaging often requires the individual to lie in a supine position. Consequently, physicians may base surgical decisions on a position that the individual does not functionally use in daily life[7].
Duffy (2019) suggests that speaking in a supine position may facilitate velopharyngeal closure due to the effect of gravity, as a behavioral intervention for resonance in some individuals with dysarthria and velopharyngeal insufficiency[8]. However, Duffy (2019) does not provide evidence to support this hypothesis[8]. Therefore, the effect of speech production in the supine position on velopharyngeal function needs to be investigated to test the gravity hypothesis. Moreover, there are concerns regarding the functionality of speech production in the supine position for patients and its social acceptability. Thus, this study uniquely aims to examine how speech production in a semi-upright 45° position, which is more functional for patients and more socially acceptable, affects velopharyngeal function. Additionally, this study is expected to provide new evidence regarding the functional appropriateness of deciding on velopharyngeal dysfunction surgery based on MRI imaging in the supine position. The purpose of this study is to compare the nasalance scores in upright, semi-upright, and supine positions in healthy individuals. Furthermore, it aims to determine whether there are statistically significant differences in nasalance scores between these positions.
Methods
Research DesignThe design of the study is a general survey model. Approval for the study's ethical compliance was granted by the Non-Interventional Clinical Research Ethics Committee of Cappadocia University on January 20, 2023, under the approval number E-64577500-050.99-35192. The study protocol was designed following the principles outlined in the Declaration of Helsinki.
Participants
A total of 70 participants, whose native language is Turkish and who are aged between 20 and 52 years, were included in the study. The inclusion criteria for the participants are as follows:
Inclusion Criteria for Participants
•Native Turkish speakers,
•Aged between 19-55 years,
•Absence of neurological conditions, craniofacial abnormalities, musculoskeletal issues, septal deviation, or swallowing impairments,
•Not having an upper respiratory tract infection at the time of assessment,
•No history of nasal, paranasal sinus, and/or oropharyngeal surgery.
Comprehensive details about the study were shared with all participants, and their informed consent was obtained.
Data Collection Tools
Demographic Information Form
This form contains information about the participants' age, gender, body mass index, height, weight, and whether they have any neurological conditions, craniofacial anomalies, musculoskeletal problems, swallowing difficulties, or upper respiratory tract infections at the time of the assessment.
Nasometer
The nasometer is an instrument that provides objective information indirectly about velopharyngeal function. The Nasometer consists of an external Nasometer II module, a separator plate with microphones above and below it, Nasometer software, and a computer. The Nasometer records acoustic energy from the oral and nasal cavities using the microphones positioned above and below the separator plate, calculating a nasalance score. The nasalance score represents the ratio of nasal acoustic energy to total (nasal + oral) acoustic energy as a percentage. In this study, the PENTAX Nasometer II 6450 was used[9].
Various passages that have been normed for Turkish are available to obtain nasalance scores[10-12]. The studies conducted by Saraç et al. (2011) and Ünal-Logacev et al. (2020) are normative studies with children[10,12]. The normative study conducted by Karakoç et al. (2013) includes adults aged 18-69[11]. Therefore, to facilitate the interpretation of the data in our study, we used the Oral, Oronasal, and Nasal passages developed by Karakoç et al. (2013). These three passages are the Turkish equivalents of the standard passages used for nasometric evaluation in English: the Zoo Passage (oral passage), the Rainbow Passage (oronasal passage), and the nasal sentences (nasal passage).
Data Collection Procedure
Data were collected between April 17, 2023, and July 1, 2023. The data collection took place in the Voice, Speech, Resonance, and Swallowing Disorders Research Laboratory at the Speech and Language Therapy Education, Practice, and Research Unit of Cappadocia University. The laboratory was specially designed to ensure sound insulation and minimize reverberation.
A preliminary study was carried out with a pilot sample of 5 participants to predict any issues or needs that might arise in the main study. As a result of the pilot study, a table was arranged for the Nasometer equipment and computer (Figure 1). The font size of the speech stimuli that participants were asked to repeat was increased.
 Büyütmek İçin Tıklayın |
Figure 1: Data collection environment |
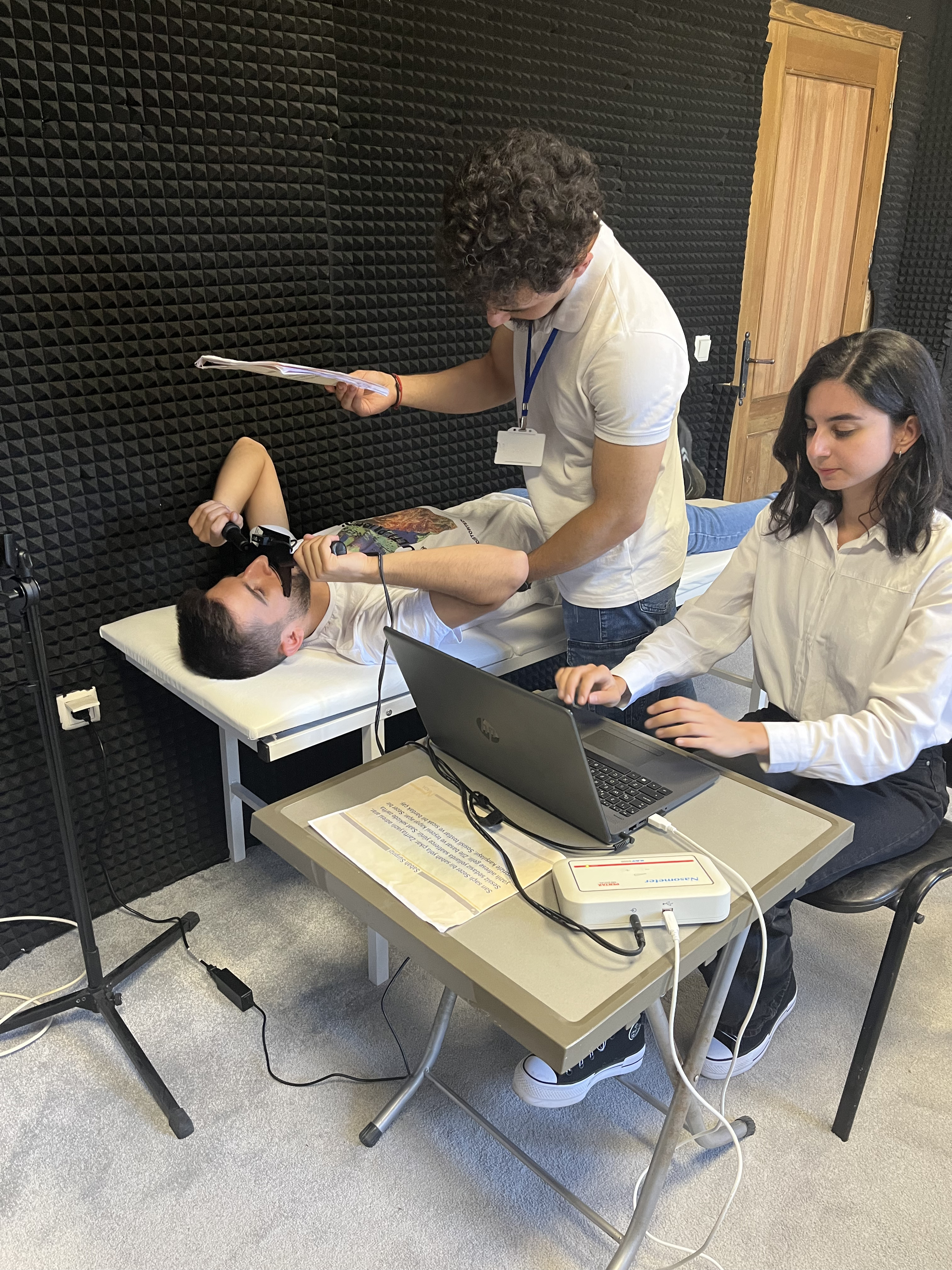
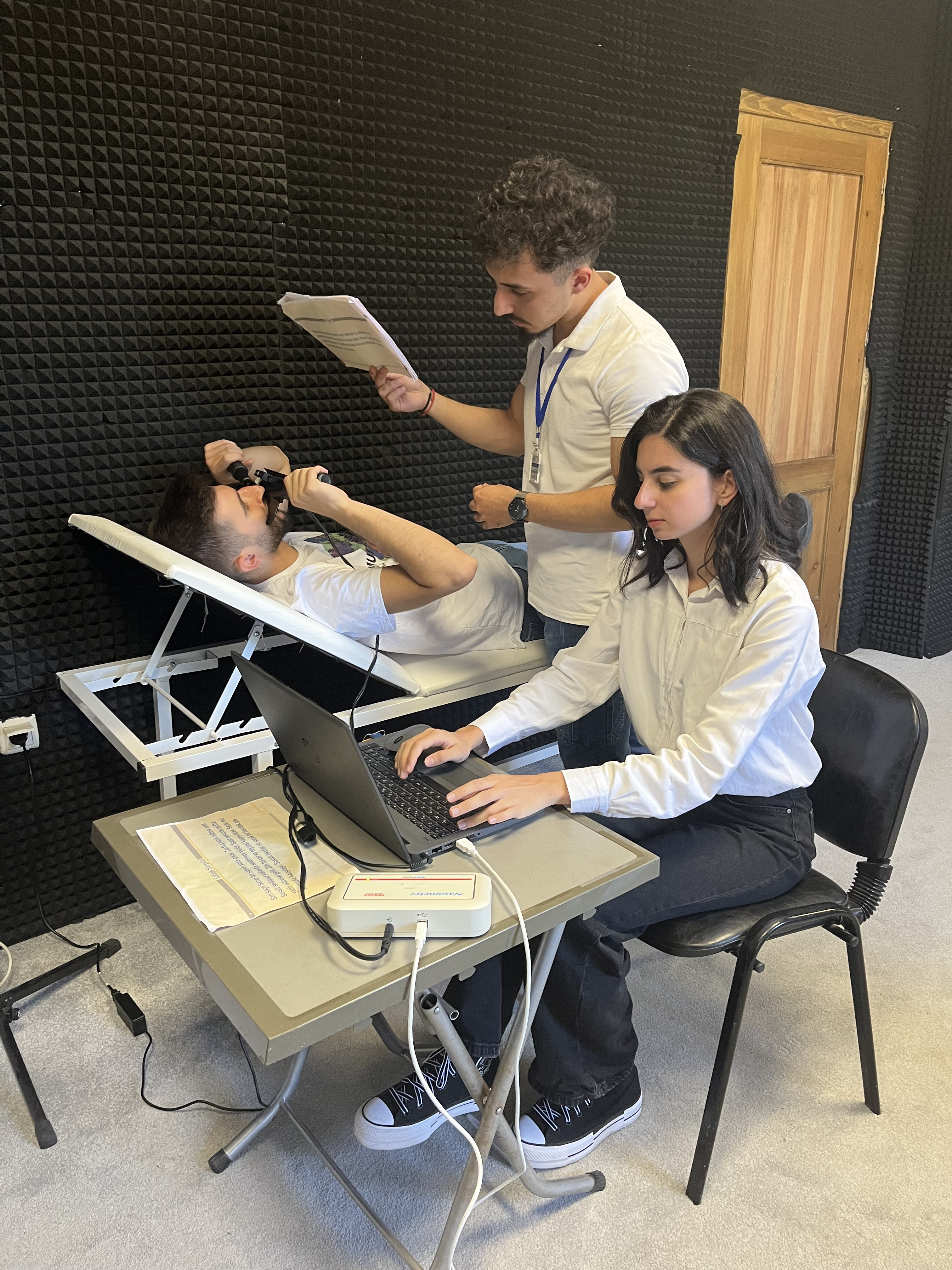
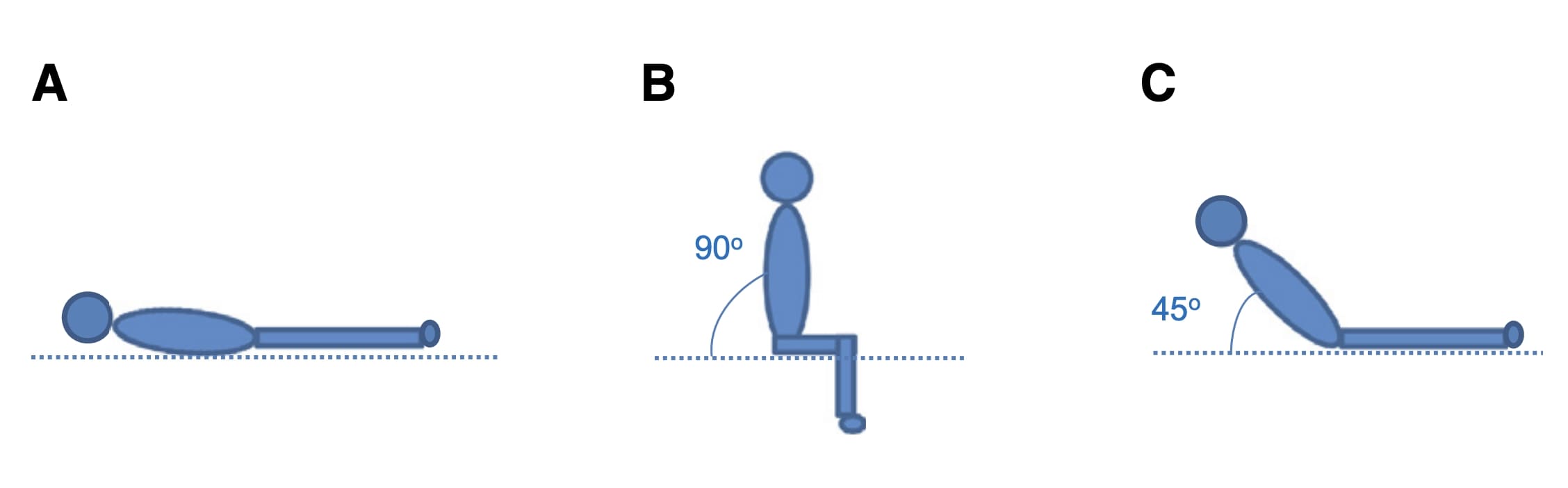
The measurement of nasalance scores was conducted using the Nasometer II 6450. The parameters of mean, minimum, and maximum nasalance scores were analyzed. The participants' positions on the adjustable stretcher were precisely calculated and adjusted using the Loyka 5522-200 digital angle gauge. The Nasometer was calibrated according to the protocols before each recording. Nasometric evaluation in the supine position was performed with the participant lying on the stretcher (Figure 2); nasometric evaluation in the upright position was done with the participant seated upright on the stretcher (Figure 3); and nasometric evaluation in the semi-upright position was conducted with the participant lying on the stretcher adjusted to a 45° angle (Figure 4) (Figure 5).
 Büyütmek İçin Tıklayın |
Figure 2: Nasalance measurement in supine position |
 Büyütmek İçin Tıklayın |
Figure 3: Nasalance measurement in upright position |
 Büyütmek İçin Tıklayın |
Figure 4: Nasalance measurement in semi-upright position |
 Büyütmek İçin Tıklayın |
Figure 5: Three different positions: (A) supine (B) upright and (C) semi-upright |
Participants were instructed not to move their heads while repeating the speech stimuli. The speech stimuli were printed horizontally and laminated for presentation to the participants. To prevent head movement, the speech stimuli were positioned at the participants' eye level. Participants were instructed to repeat the speech stimuli at a normal speed.
Data Analysis
The data were processed and analyzed using IBM SPSS 27.0 software. Descriptive and inferential statistical techniques were utilized. In descriptive statistics, mean, standard deviation, frequency, and percentage were used. In inferential statistics, a significance level of p < .05 was set. Before comparing the participants' measurements in the upright, semi-upright, and supine positions, the normality of the data was tested using the Kolmogorov-Smirnov Test, histograms, skewness, and kurtosis values. Since the data were not normally distributed, the Friedman Test was used. To determine which groups contributed to the significant difference, the Wilcoxon Signed-Rank Test with Bonferroni correction was applied. In the Wilcoxon Signed-Rank Test, a significance level of p < .017 with Bonferroni correction was accepted.
Results
The demographic characteristics of the participants are presented in Table 1.){kind=link}
Table 1: Demographic Characteristics of Participants (n=70)
The comparison of the participants' average nasalance scores in the supine, semi-upright, and upright positions for oral sentences is shown in Table 2. A statistically significant difference was found between the nasalance scores in the supine, semi-upright, and upright positions for the text composed of oral sentences (χ2(2)=33.412, p<.001). This difference was found to be due to the nasalance scores between the supine and semi-upright positions (Z= -5.259, p<.001) and between the supine and upright positions (Z= -4.035, p<.001).
){kind=link}
Table 2: Comparison of Nasalance Scores in Different Positions for Oral Passage (n=70)
The comparison of the participants' average nasalance scores in the supine, semi-upright, and upright positions for oronasal sentences is presented in Table 3. A statistically significant difference was found between the nasalance scores in the supine, semi-upright, and upright positions for the text composed of oronasal sentences (χ2(2)=27.871, p<.001). This difference was attributed to the nasalance scores between the supine and semi-upright positions (Z= -4.864, p<.001) and between the supine and upright positions (Z= -2.534, p<.001).
){kind=link}
Table 3: Comparison of Nasalance Scores in Different Positions for Oronasal Passage (n=70)
The comparison of the participants' average nasalance scores in the supine, semi-upright, and upright positions for nasal sentences is shown in Table 4. A statistically significant difference was found between the nasalance scores in the supine, semi-upright, and upright positions for the text composed of nasal sentences (χ2(2)=14.625, p<.001). This difference was found to be due to the nasalance scores between the supine and semi-upright positions (Z= -4.452, p<.001).
){kind=link}
Tablo 4: Comparison of Nasalance Scores in Different Positions for Nasal Passage (n=70)
Discussion
This study aimed to explore the impact of body position-supine, semi-upright, and upright-on nasalance scores in healthy individuals. The findings reveal significant differences in nasalance scores across different positions, with the supine position consistently showing lower scores compared to the upright and semi-upright positions. This supports previous studies that have demonstrated the influence of gravity on speech structures, particularly in the velopharyngeal mechanism[5,13].One of the critical aspects of our results is the consistency with past research, which has highlighted that gravity influences velopharyngeal structures, affecting the functional capacity for speech production. Broadwell et al. (2015) specifically explored the aerodynamic characteristics of speech in upright and supine positions, showing a decrease in nasalance scores in supine positions[13]. In this study involving 37 participants, pressure flow rate and nasalance scores were analyzed in both positions. Although no significant difference in pressure flow rate was found between the two positions, a significant decrease in some nasalance scores was observed in the supine position. Broadwell et al. (2015) reported that the supine position led to a decrease in certain nasalance scores compared to the upright position, mirroring the trends found in this study[13]. The movement of the soft palate in the supine position, as observed by Kitamura et al. (2005), also correlates with the changes in nasalance scores, suggesting that altered velopharyngeal function may be driven by gravitational effects[3]. Kitamura et al. (2005) observed that the tongue, soft palate, and lips were positioned further back in the supine position compared to the upright position, likely due to the effects of gravity[3]. This retraction could explain the reduced nasalance scores we observed in the supine position, as gravitational forces may limit velopharyngeal closure. Specifically, the backward retraction of the soft palate in the supine position, observed by Sutthiprapaporn et al. (2008), may contribute to the reduced resonance seen in our results[5]. Sutthiprapaporn et al. (2008) examined the effect of gravity on oropharyngeal structures in upright and supine positions with seven participants, concluding that the positions of the oropharyngeal structures varied depending on gravity[5]. Perry (2011) conducted a study with five healthy adult female participants to compare the velopharyngeal structures in upright and supine positions[14]. The results showed significant differences in velar height, although no notable differences were observed in the length or thickness of the velum. These findings are consistent with our results, as the upright position consistently yielded higher nasalance scores, likely reflecting more effective velopharyngeal closure due to reduced gravitational constraints. Kollara and Perry (2013) compared the velopharyngeal structures of 12 typically developing children aged 4 to 8 years in upright and supine positions[4]. Their results indicated that while the thickness and height of the velum remained almost the same in different positions, its length consistently increased. Although our study focused on adults, the consistent reduction in nasalance scores in the supine position supports the notion that velopharyngeal adjustments occur in response to gravitational forces. Engwall (2003), using magnetic resonance imaging (MRI) with a single participant, examined the impact of gravity on tongue position and found no significant change in tongue position between supine and prone positions[2]. The difference between Engwall's findings and ours may be due to their study's sample size, which included only one participant. Additionally, our study specifically focused on the functional dynamics of velopharyngeal structures, which may account for the observed differences in results.
The significant difference between supine and semi-upright positions is particularly noteworthy. Previous studies have mostly compared upright and supine positions, but our study contributes novel data by including a semi-upright posture. This position, often used in clinical settings, offers more functional insight into everyday speech production, where individuals are rarely fully supine. As the semi-upright position showed intermediate nasalance scores, it may provide a more realistic representation of natural velopharyngeal function for clinical evaluations.
Additionally, the variations in nasalance scores across different phonetic contexts suggest that body positioning affects different speech sounds to varying degrees. The more significant changes in oral passages compared to nasal ones may be due to the role of velopharyngeal closure being more critical for non-nasal sounds[7].
Future studies should explore these findings in clinical populations, particularly those with dysarthria and velopharyngeal dysfunction, to determine the practical implications of body position in therapeutic contexts. Additionally, examining other intermediate body positions could provide further insight into optimizing clinical assessment protocols.
Conclusion
This study demonstrates that body position significantly influences nasalance scores in healthy individuals. These results have important implications for clinical assessments of velopharyngeal function, especially in contexts such as resonance disorders or velopharyngeal dysfunction surgeries. Clinicians should consider body positioning when making diagnostic or surgical decisions to ensure that assessments reflect functional, everyday speech production.
Acknowledgments
This study was produced from the data obtained from the project supported by TÜBİTAK 2209-A - University Students Research Projects Support Programme, project number 1919B012220729. The authors would like to thank the Scientific and Technological Research Council of Türkiye (TÜBİTAK) for their contributions.
Data Availability Statement
The datasets utilized and/or examined during the present investigation can be obtained from the corresponding author upon a reasonable request.
Declaration of Interest
The authors have no conflicts of interest to declare.
Ethics Committee Approval
The ethics committee decision for the research was taken at the Cappadocia University Non-Interventional Clinical Research Ethics Committee meeting held on January 20, 2023. (Approval number: E-64577500-050.99-35192).
Informed Consent
Written and verbal informed consent was obtained from the participants who agreed to take part in the study.
Funding
This study was financially supported by the Scientific and Technological Research Council of Türkiye (TÜBİTAK) under the 2209-A University Students Research Projects Support Programme, with project number 1919B012220729.
Reference
1) Varol T, Tuğlu Mİ, Vatansever S, Cezayirli E, Tatlısumak E, Hayretdağ C. Stereological, Morphological and Histochemical Study on the Effect of Hypergravity on Newborn Rat Brain. Ege Tıp Dergisi. 2004;43(3):143-149.
2) Engwall O. A revisit to the Application of MRI to the Analysis of Speech Production-Testing our assumptions. 2003:43-48.
3) Kitamura T, Takemoto H, Honda K, et al. Difference in vocal tract shape between upright and supine postures: Observations by an open-type MRI scanner. Acoustical Science and Technology. 2005;26(5):465-468.
4) Kollara L, Perry JL. Effects of gravity on the velopharyngeal structures in children using upright magnetic resonance imaging. Cleft Palate Craniofac J. 2014;51(6):669-76. [ Özet ]
5) Sutthiprapaporn P, Tanimoto K, Ohtsuka M, Nagasaki T, Iida Y, Katsumata A. Positional changes of oropharyngeal structures due to gravity in the upright and supine positions. Dentomaxillofac Radiol. 2008;37(3):130-5. 7) Perry JL, Sutton BP, Kuehn DP, Gamage JK. Using MRI for assessing velopharyngeal structures and function. Cleft Palate Craniofac J. 2014;51(4):476-85. [ Özet ]
8) Duffy JR. Motor Speech Disorders: Substrates, Differential Diagnosis, and Management. 4th ed. Mosby Elsevier; 2019.
9) Kummer AW. Cleft Palate and Craniofacial Conditions: A Comprehensive Guide to Clinical Management. 4th ed. Jones & Bartlett Learning; 2018.
10) Sarac ET, Kayikci ME, Ozkan S. Nasality evaluation of Turkish phonemes in vowel-consonant combinations. Int J Pediatr Otorhinolaryngol. 2011;75(7):894-8. [ Özet ]
11) Karakoc O, Akcam T, Birkent H, Arslan HH, Gerek M. Nasalance scores for normal-speaking Turkish population. J Craniofac Surg. 2013;24(2):520-2. [ Özet ]
12) Ünal-Logacev Ö, Kummer AW, Çetin C, Topbaş S. Nasometric evaluation of resonance disorders: A norm study In Turkish. Int J Pediatr Otorhinolaryngol. 2020;131:109888. [ Özet ]
13) Broadwell KR, Perry JL. Aerodynamic Speech Characteristics in Upright and Supine Positions. Contemporary Issues in Communication Science and Disorders. 2015;42(Fall):173-181.
14) Perry JL. Variations in velopharyngeal structures between upright and supine positions using upright magnetic resonance imaging. Cleft Palate Craniofac J. 2011;48(2):123-33. [ Özet ]